Whilst DID and OSDD-1 are not presently classified as spectrum disorders, as they exist as separate diagnoses, the presentation of dissociative symptoms related to the diagnoses could be visualised as a spectrum of different symptoms ranging from “normal” experiences to sub-clinical experiences to clinical experiences.
The Multidimensional Inventory of Dissociation (MID) is one of the more accessible comprehensive measurements of dissociative symptoms, it consists of 218 questions covering multiple scales pertaining mostly to dissociative and post traumatic experiences, the answers are self reported however the administering person may make adjustments to scoring where they see fit. These answers may then be inputted into the MID Analysis excel program, where a report is automatically generated with suggestions towards diagnosis as well as details of individual subcomponents’ scoring.
For the purspose of considering DID/OSDD from a spectrum perspective, the aspects we will be considering are as follows
– General Patient Dissociative Symptoms
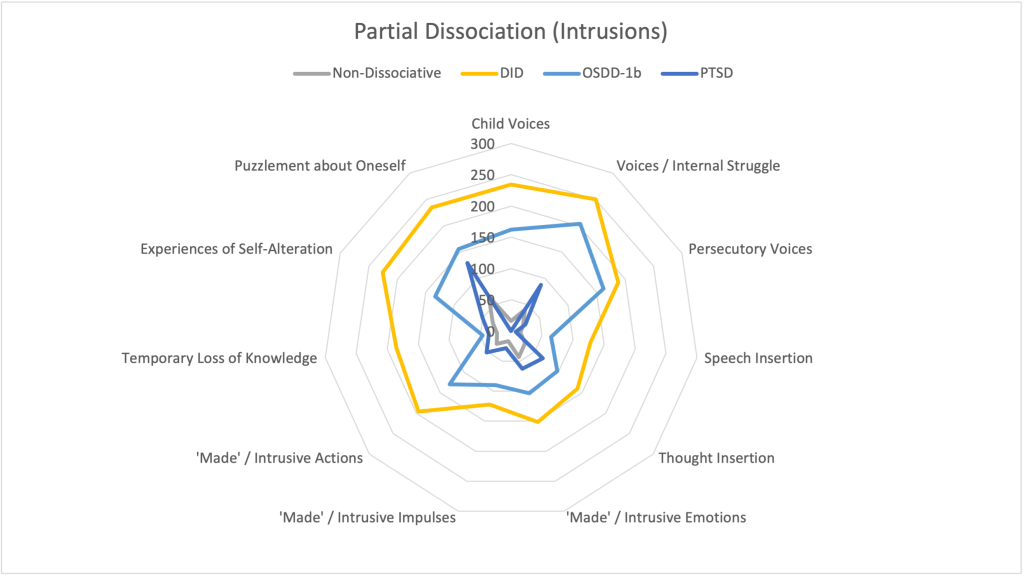
– Partially-Dissociated Intrusions
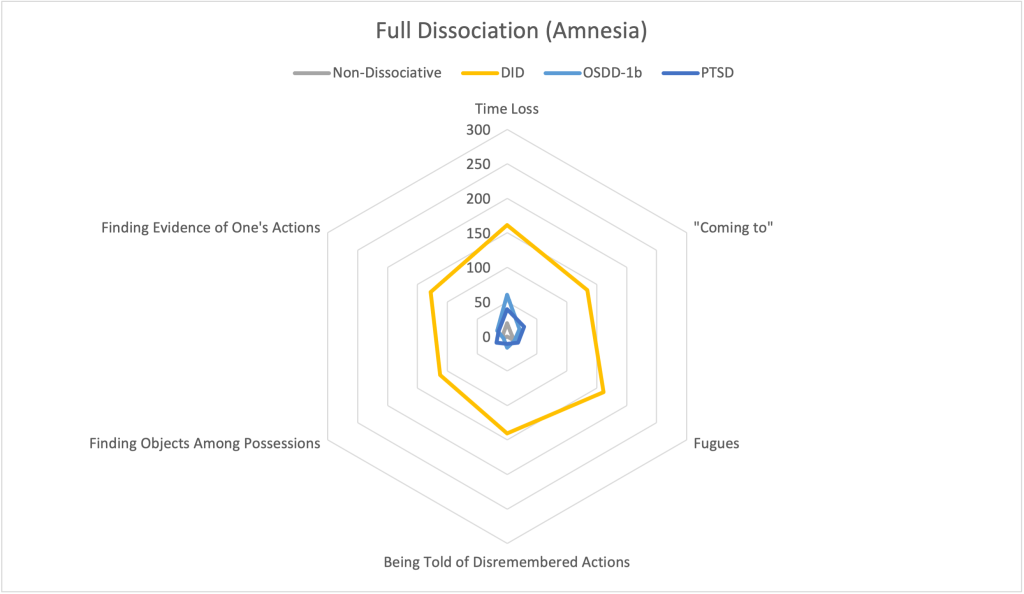
– Fully-Dissociated Actions
There also exists Validity scales as well as measurements of Functioning and Impairment, these influence the results reported by the MID, however they do not directly pertain to symptoms of dissociation, thus they have been omitted for simplicity of analysis.
The below charts depict the average or “norm” scoring of non-dissociative, DID, OSDD-1b, and PTSD test takers based on the data provided in v5.2 of the MID Analysis. The charts use a scale of clinical significance, where a score of 100 or higher on any one measurement is considered clinically significant, and is scaled linearly such that a score of 200 is twice as significant as a score of 100.
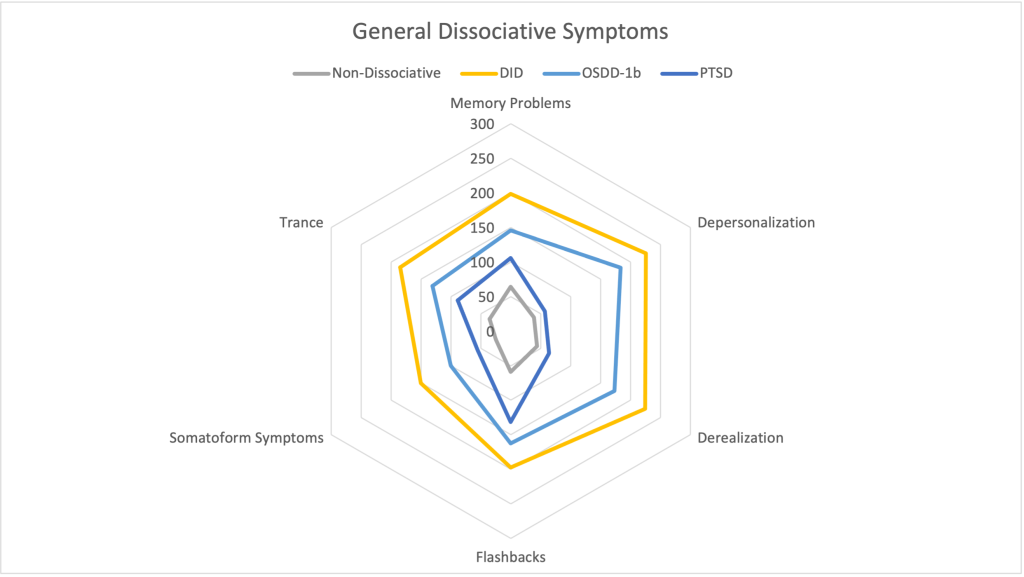
Note:These charts do not include series for OSDD-1a specifically. Whilst the MID does make some considerations towards the continuity in sense of self and agency that the DSM-V refers to, it does not necessarily measure the distinction between alters / personality states referenced in the DSM-IV. Additionally the normed values for the OSDD measurement specifically include the lessened amnesia criteria, such that indviduals with OSDD-1a may be identified as having DID using these measurements, this emphasises the importance of clinical judgement when assessing patients.
Visualising the Spectrum
Sandra L. Paulsen, working off of J.G. Watkins’ prior Ego-State/Dissociative work, devised the following Dissociative Continuum, focusing on the inner conflict and sense of self/selves. This ranges from the normal “part of me wants to do this but another part of me doesn’t” that might arise from regular inner conflict, unrelated to separated senses of self, to DID where the parts are disintegrated and have separate senses of self:

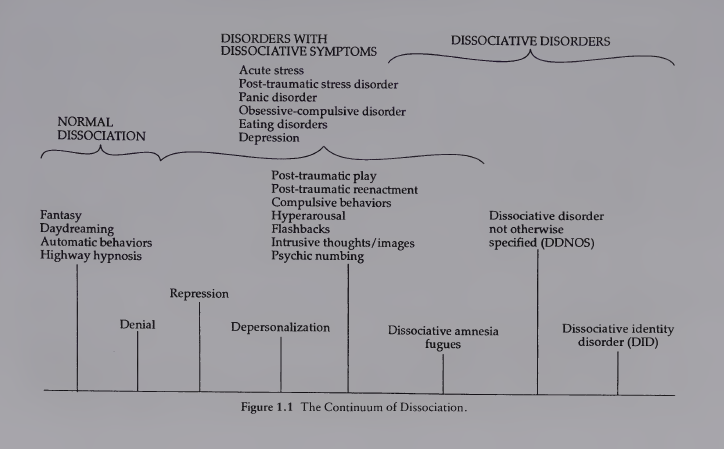
Lynda Shirar’s book Dissociative Children: Bridging the Inner and Outer Worlds presents a slightly more detailed continuum, displayed below.
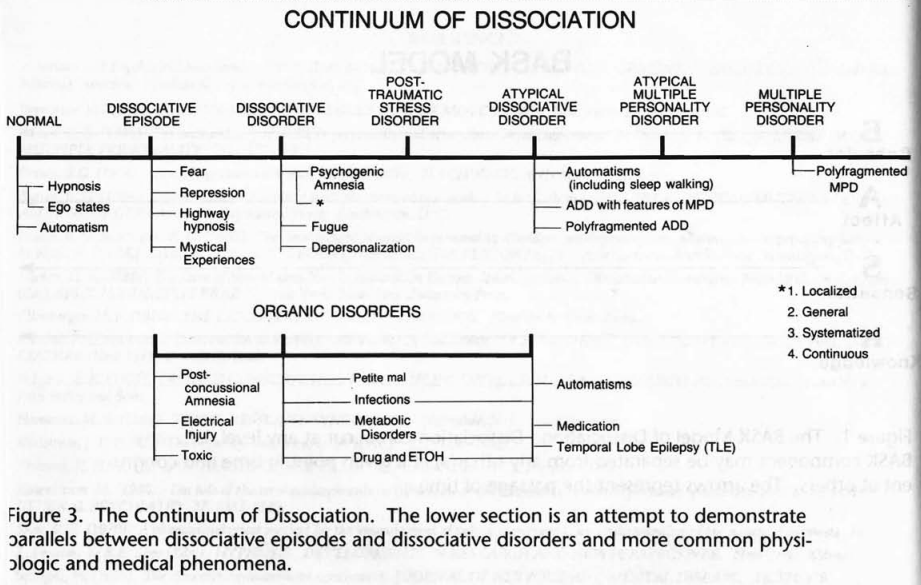
A similar but more detailed continuum, is that of the BASK model of dissociation, pictured below, where Atypical Dissociative Disorder and Atypically Multiple Personality Disorder is representative of OSDD-1a/b and Multiple Personality Disorder is representative of DID.
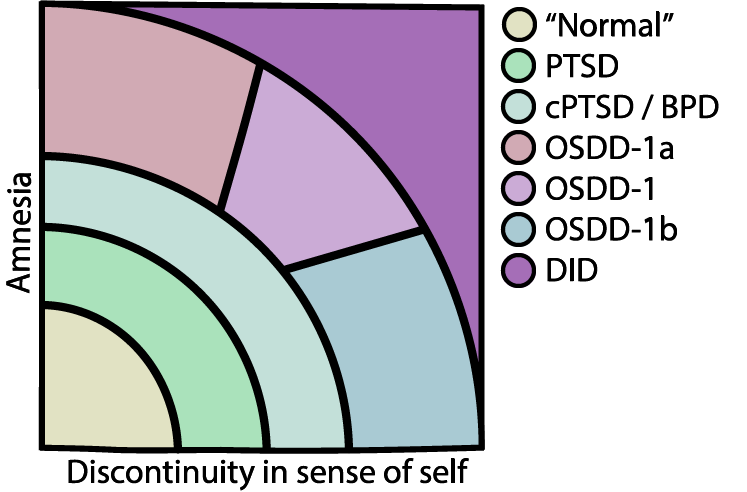
Another perspective one can take for looking at dissociation in DID/OSDD as a spectrum, would be taking the two differing criteria within OSDD-1a and OSDD-1b (The less than marked discontinuities in sense of self and agency against the lack of narrative amnesia) and plotting them against each other, which would likely vaguely resemble the below chart: